
Q. 53, 54, 55 - Quality of Life and "long-term" COVID-19
LTCOVID.com
Thanks for visiting!
To translate this page, select your
language from the dropdown menu below:
These three questions are essentially one question, so grouped together here.
It makes sense that being sick doesn't feel good; doesn't add much if anything that is clearly positive to one's existence.
It makes sense that although many things contribute to one's Quality of Life (QoL), losing one's health may quickly make those other things seem less important contributors.
We asked about their perceptions of Quality of Life from those who identify as "long-term" COVID-19 patients.
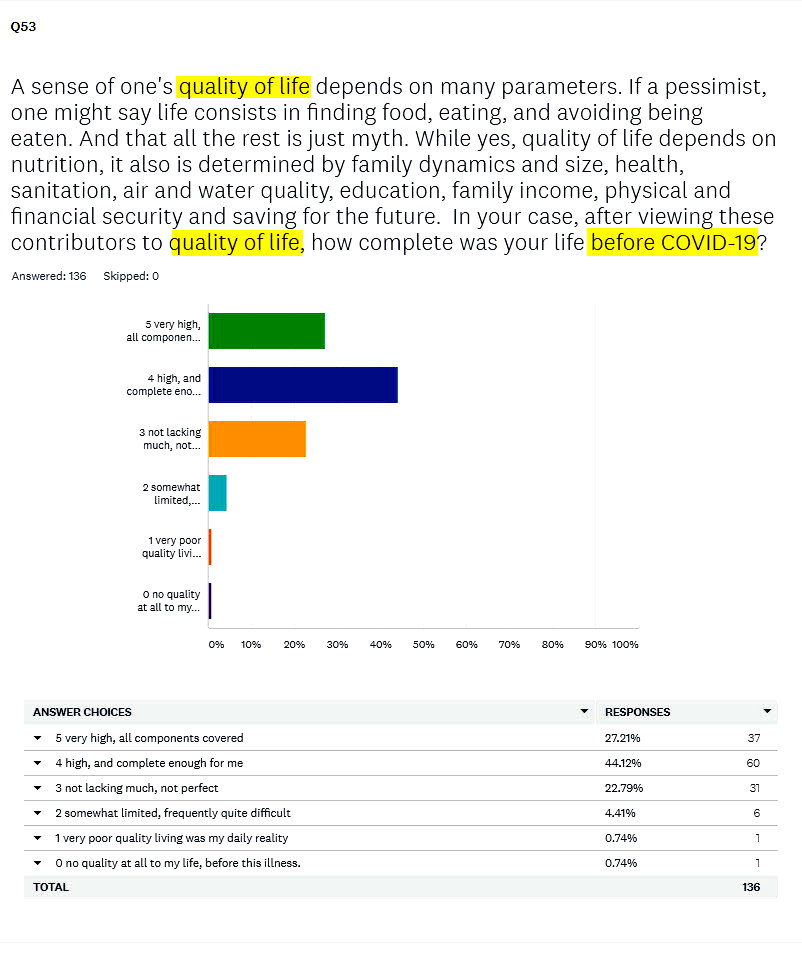
(Q. 53) How did they view QoL BEFORE becoming ill?
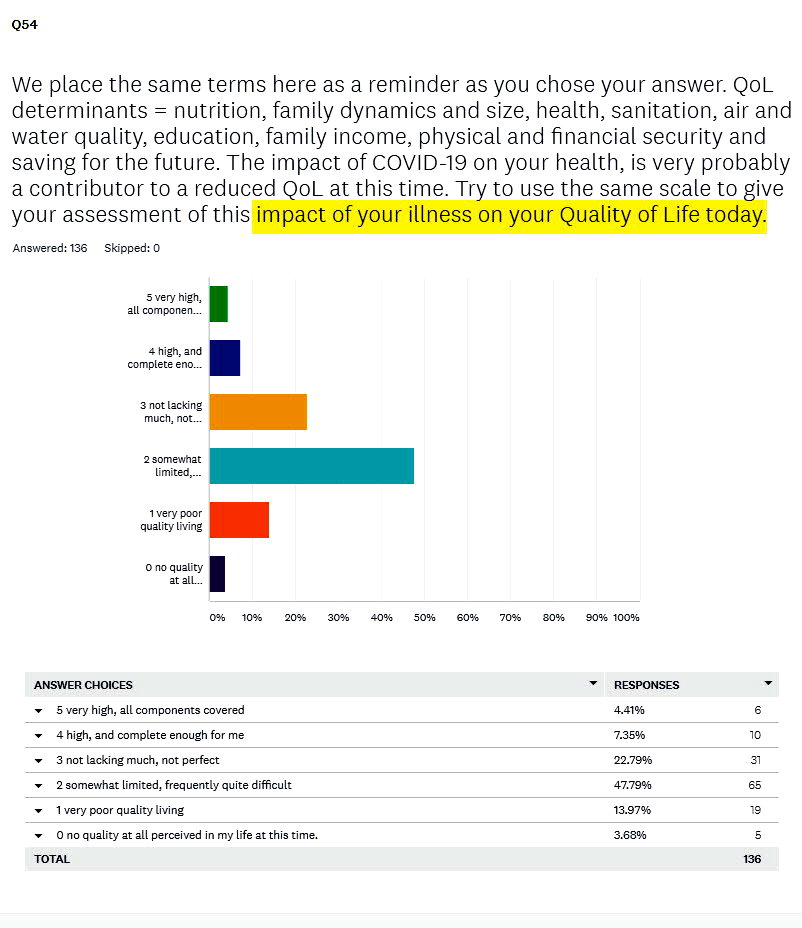
(Q. 54) How about DURING the illness as they responded to a questionnaire?
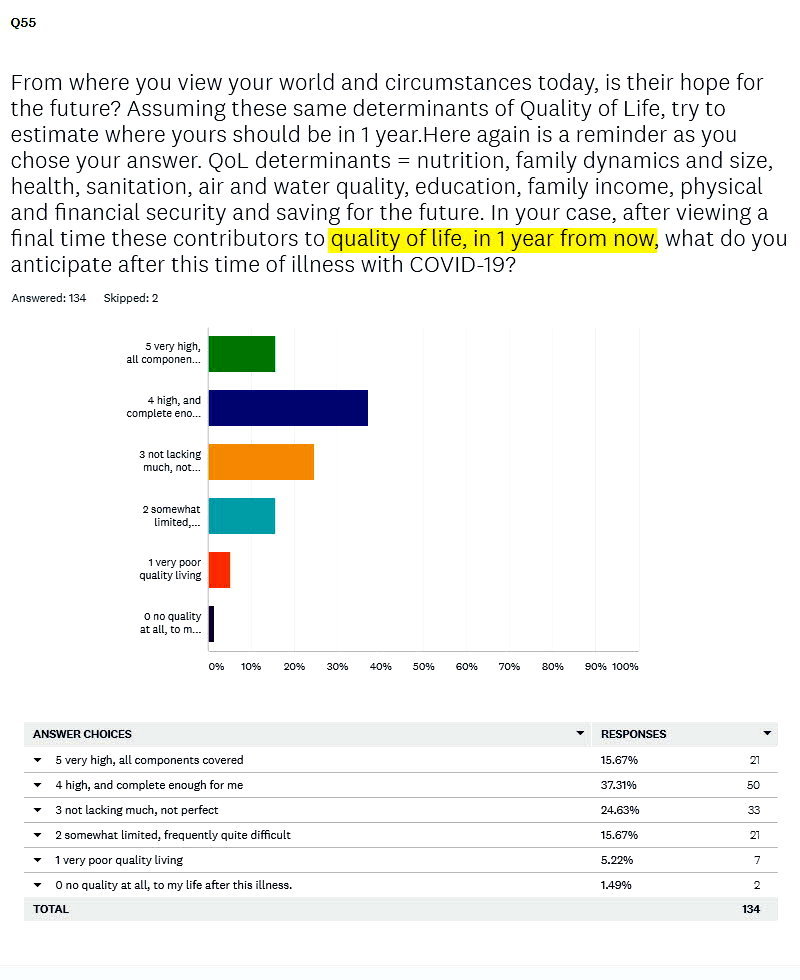
(Q. 55) And how would they project their Quality of Life at 1 YEAR into the future?
Here the three questions, to see how phrased, and the responses that returned:
Placed together here to simplfy their revies, these questions look like this:
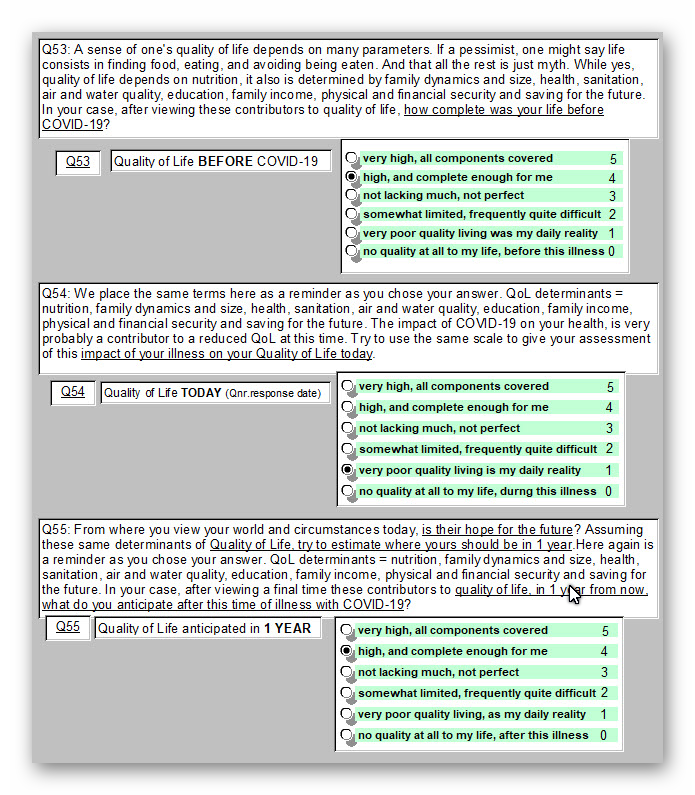
- Above are also shown one person's responses.
- Response options were scored from a maximum QoL of 5, to no QoL at 0, and as shown. This permitted subsequent quantitative summary and analysis. These are referred to below as QALYs or quality points.
- It may not seem that a change from 4 to 1 QALYs is a large change. Yet it probably is. For instance: 4, QoL "high, and complete enough for me," to 1, QoL "very poor quality living, as my daily reality." That is clearly a major change in the quality aspects of that persons existence.
- Responses were obtained at a single time along with the rest of the questionnaire, and not at the three times requested through the 3 questions. (Before, During, & In 1 Year). So responses for Before & I Year are based on recall of the past (6 months ago), and projection or anticipation of the future (at 1 year).
--------
Summarizing these responses mathematically provides some useful insights.
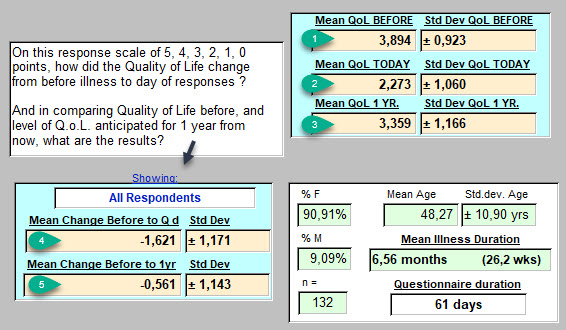
As shown, the values generated here represent the entire sample, minus 3 unsuitable questionnaires, so n = 132, and no respondent skipped these two questions.
Since this is essentially a Likert scale from 0 to 5, if responses are normally distributed, a midpoint of 2.5 can be anticipated for the means of these QALYs.
-
- 132 respondents, 90.9% female with an average age of 48.3 years (range 17.1 to 72.3).
- Illness duration : 6.56±1.615 months, or 26.24±6.46 weeks.
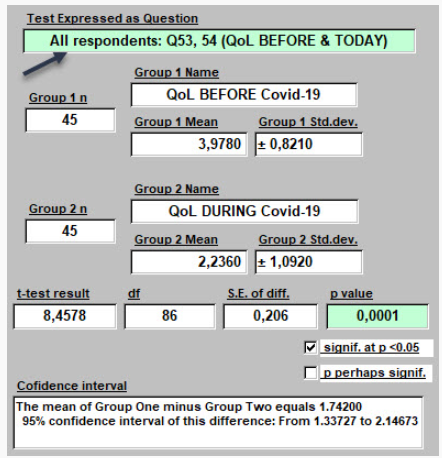
- On this 0 to 5 Likert scale, BEFORE becoming ill, the mean value is 3.894±0.923, shown at green number 1 above. That's above the midpoint of this theoretical distribution of 2.5.
- On the day of response, DURING the illness for most, the mean is 2.273±1.060 (at green #2)
- Projected 1 YR into the future, this sample's answers generate a mean of 3.359±1.166 QALYs.
- At green #4 on the left above, from BEFORE to DURING illness -1.621±1.171 QALY points lost.
- From BEFORE this illness to 1 YR in the future, a mean of -0.561±1.143 QALY points lost.
As suggested above, small mathematical changes on these scales, may imply important changes in perceived Quality of Life.
Analysis of Results:
Some readers may simply "eyeball" the results and move towards an interpretation.
Comparison of several of these mean values may be of use. Possibly adding confirmation to impresseion.
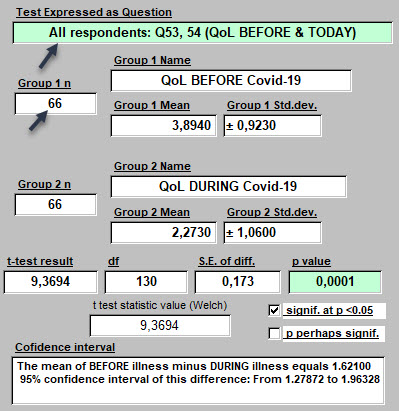
- These are results of Student's t-test, paired, since both responses come from the same respondent (i.e., not comparing males with females, but two answers from the same person). That is why the n value of 132 respondents became 66 as seen above when challenging these means with Student's test.
- The loss of Quality of Life from BEFORE to DURING this illness was very significant.
- With a p value = 0.0001 that suggests that there is only 1 chance in 10 000, that this hypothesis of a loss of quality in life is false. It's probably true.
- With 95% confidence, that amount of loss of quality in life due to this illness, varied from 1.28 to 1.96 QALYs for these respondents.
Interpretation:
-
-
- This may be a confirmation of suspicions for some, but not a surprise.
- "Long-term" COVID-19 is a major illness: lasting a very long time, and with many symptoms reported (see other responses for Q. 38, 39, 40). At time of response, these individuals reported a mean of 12.62±7.13 symptoms. (And yet, they still responded! Thank you! )
- So a loss on average of 2 steps down in Quality of Life, and as confirmed statistically here a difference of 1.6 steps, is a major loss. Seemingly undeniable.
-
One may have the thought, that even without statistical confirmation, being sick is no fun, and Quality of Life, no matter how defined, will obviously suffer during any serious illness.
---------
We can never get back to the past exactly as it was. And perhaps shouldn't try.
But if one enjoyed one's Past Quality of Life, as sensed overall and combined into a single answer here,
most might assume that after this illness has passed and one has recovered, that previous QoL could also be recovered.
Is that the case?
Do those with "Long-term" COVID-19 anticipate a full return to Quality of Life?
From the result presented above, it may not be so.
We are not trying to predict the future here.
We are simply presenting how these respondents felt on the day they answered, about possibilities : about the potential for improvement after a little time has passed.
Here is the Analysis of those Results: BEFORE compared with in 1 YR
These are of course, the same 132 respondents.
None skipped Q. 53. Two skipped Q. 55.
Again, each paired with self. So we'll use n = 66 for BEFORE, and n = 65 for 1 YR.
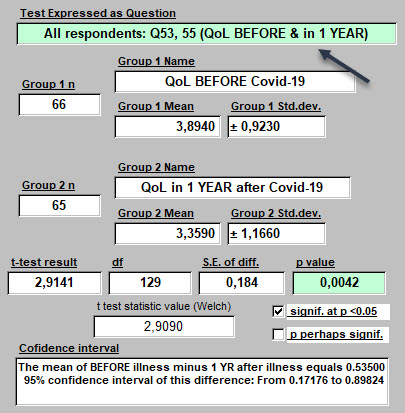
- Comparing means for Quality of Life BEFORE, and in 1 YEAR, respondents anticipate losing a mean of -0.561±1.143 QALYs. (green #5 presented above)
- With 95% confidence, that ranges from 0.17 to 0.90 QALYs.
- How certain is that? That the anticipated future, will have less Quality of Life, than did life lived before COVID-19?
- The p value is 0.0042. Statisticians would say the difference in these mean values is significant because it's below 0.05. Another way of saying it is that there are only 42 chances out of 10 000, (ten thousand) that this apparent difference is not real, not present. Just an imaginary co-incidence. Well, not very likely.
- Again, we are not predicting the future here, or trying to. We are trying to add clarity to better understand the future anticipated by residents on the day they took the questionnaire. This answer obtained at a mean of 26.2 weeks into their illness.
Interpretation:
-
- Clearly, less Quality of Life is anticipated for the future, when compared with known QoL in the past.
- Some answered that there would be no change in past and future life quality.
- But of 37 who responded a level 5 QALY BEFORE, only 13 (35%) anticipated a QALY level 5 at 1 YR.
- Of 60 who responded a level 4 QALY BEFORE, only 25 (41.7%) anticipated a QALY level 4 at 1 YR.
- No one suggested life would be improved by this illness.
COMMENT 1
Some may ask if having a larger sample might make this apparently certain result, just disappear?
A preliminary analysis had been presented elsewhere when the sample size was 89.
Here were the means:
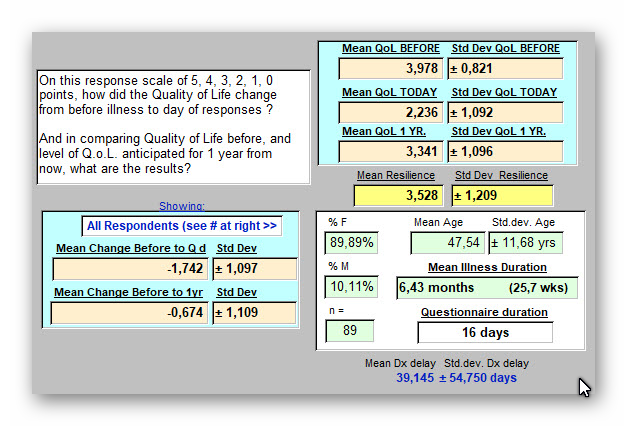
And here the statistical challenge of those results:
The conclusion was already the same.
Adding the responses for n = 132 respondents has only changed the level of certainty of the result.
But its conclusion has not changed.
Given the strength of the result at our current level, adding more respondents does not seem indicated.
---------
COMMENT 2
And yet, there are experts in the field who might suggest that for some, Quality of Life may be better than anticipated by our sample when each person answered. Not worse.
- Other comparisons could be made and will be subsequently: gender differences in perceiving Quality of Life, for example. Enough has been presented here to think about.
- How does one anticipate a cheerier future? One hopes for it. And how we hope, if done successfully, is not just done willy-nilly without a plan. There can be a method. Often unconscious perhaps. At times, intentionally pursued, learned from others. At times, supported by someone else. WIth corrections made along the path as the need arises.
- So can we translate the above result (and it seems pretty certain statistically speaking) into some degree of hopelessness for the average respondent to these three questions?
- If so, that may be a place to start now, today, to make inroads into helping to boost hopefullness. Yes, even while still feeling crummy.
- There are experts in this pursuit. I am not one. Not because I am not hopeful personally for the future Quality of my Life and that of others. I tend to remain quite so, which here is anecdotal.
- But there is a path to follow on that walk from "hopelessness" to arrive at "filled with hope." And sometimes, taking a beating in life, may ultimately lead to being even more filled with hope than we were before the hard times arrived. Sounds a bit like Post Traumatic Stress Disorder (PTSD).
Heading in that positive direction, might just start here. With a review of some experts in this.
Optimism is an effective antidote for depression and self-pity. But supporting such optimism is also part of what professional help is about. Or should be.
And I take this occasion to share again my concern that Online Groups, Family, and Personal Habits might not be enough to get a person with "long-term" COVID-19 to a position of hopefulness for the future? The relation with healh-care providers seems badly damaged as already shown, and as again suggested in questions that will soon follow. And therapists? As seen in the same analysis of efficient sources of emotional support, they are not in the picture for the majority of our respondents.
Answering why is a separate study from this one.
Why might these not be ideal?
Because we have been defining here an illness which is too important, too present in the lives of too many, to think that other than a professional approach will consistently provide a cure without further delay.
Sharing anecdotes online may be nice but too often ineffective and most probably inefficient.
Sharing useful information online that points to an effective potential source of help is a different story.
Advanced here is the hope that that may be the case for this questionnaire and its analysis presented herein. One or more steps in the right direction.
-----------
<<<< Previous page
Q. 56 - Resilience and "long-term" COVID-19 >>>>>
A découvrir aussi
- Q.19 - Date illness began (2nd asking)
- Q. 32 - Are you currently more attuned to changes in physical status ?
- Q. 51 - Response of employers to respondent's illness