
Mitochondria & COVID-19 : stepping stones from the "peer-reviewed" literature
LTCOVID.com
Thanks for visiting!
To translate this page, select your
language from the dropdown menu below:
We have now presented: our "long-term" COVID-19 questionnaire. Responses and several interpretations of these, question by question, have been offered.
A hypothesis of this illness having close and important links to acquired mitochondrial diseases in this sample of respondents has been voiced.
Is there support for this hypothesis?
Below are several references, offered with short summaries of their content and/ or conclusions.
-----------
An Opening Comment.
One ultimate judge of the severity of an illness is the Pathologist.
Most of us would like to avoid a consultation with this expert to review the findings present in our personal organs and tissues, for as long as possible.
The respondents to our have presented us with a whole host of symptoms. These involve a large number of organ systems. Many practicing Medicine today, lean towards labelling these lists as unbelievable. That's unfortunate. Both for them, but especially their patients. As these findings get repeated, over and over again, that is likely to improve and the impasse may disappear.
When a patient in an ICU setting has lost the normal function of 3 organ systems, they very often are not going to make it out alive.
And in our total respondent sample, they are presenting 6.398±3.158 organ systems involved with the "long-term" COVID-19 illness. They are still walking, talking, and answering questionnaires.
Doing so even if feeling "markedly fatigued" and with a "brain fog" for the last 6.5 months. On average, 6.4 organ systems involved. How can that be?
The "long-term" variant of the COVID-19 illness represents a very widespread involvement of human organs, tissues and cells. This involvement can vary markedly (which is fortunate) in severity. So our respondent sample represents a subset of the larger COVID-19 population. We discovered that they have a "moderate illness."
How does the "Path Report" as we used to call it in the past, help to put this in perspective?
We would use this document to help us learn why a patient of ours had not had the outcome desired.
And especially, to learn those things that might permit us to do better with the next patient, presenting with the similar problem(s) and challenge(s) for us.
To attend a patient's autopsy was always a learning experience.
It was always more than discovering if there were things that we had missed or not, and that might have made a difference. It was a last sign of respect for our patient. Today, this seems to happen less often, but not because there are fewer deaths.
So below, read quietly and respectfully to learn what the Pathologist is trying to teach us about the illness caused by the SARS-CoV-2 virus.
The four horsement of a viral Apocalypse - the pathogenesis of SARS-CoV-2 infection and COVID-19
---------
Our Mitochondria and COVID-19 Bibliography
We have been "pitching" our hypothesis that the illness we studied through our questionnaire, has a strong link to mitochondrial structure and function. That COVID-19 in its "long-term" form, could be listed among other mitochondrial diseases that we also summarized.
Is there support for this hypothesis in the "peer-reviewed" literature? A literature which so many take as the ultimate sign of approval of one's work, by the voices of Science. (Not infrequently, that approval is of questionable value, but let's pass on that).
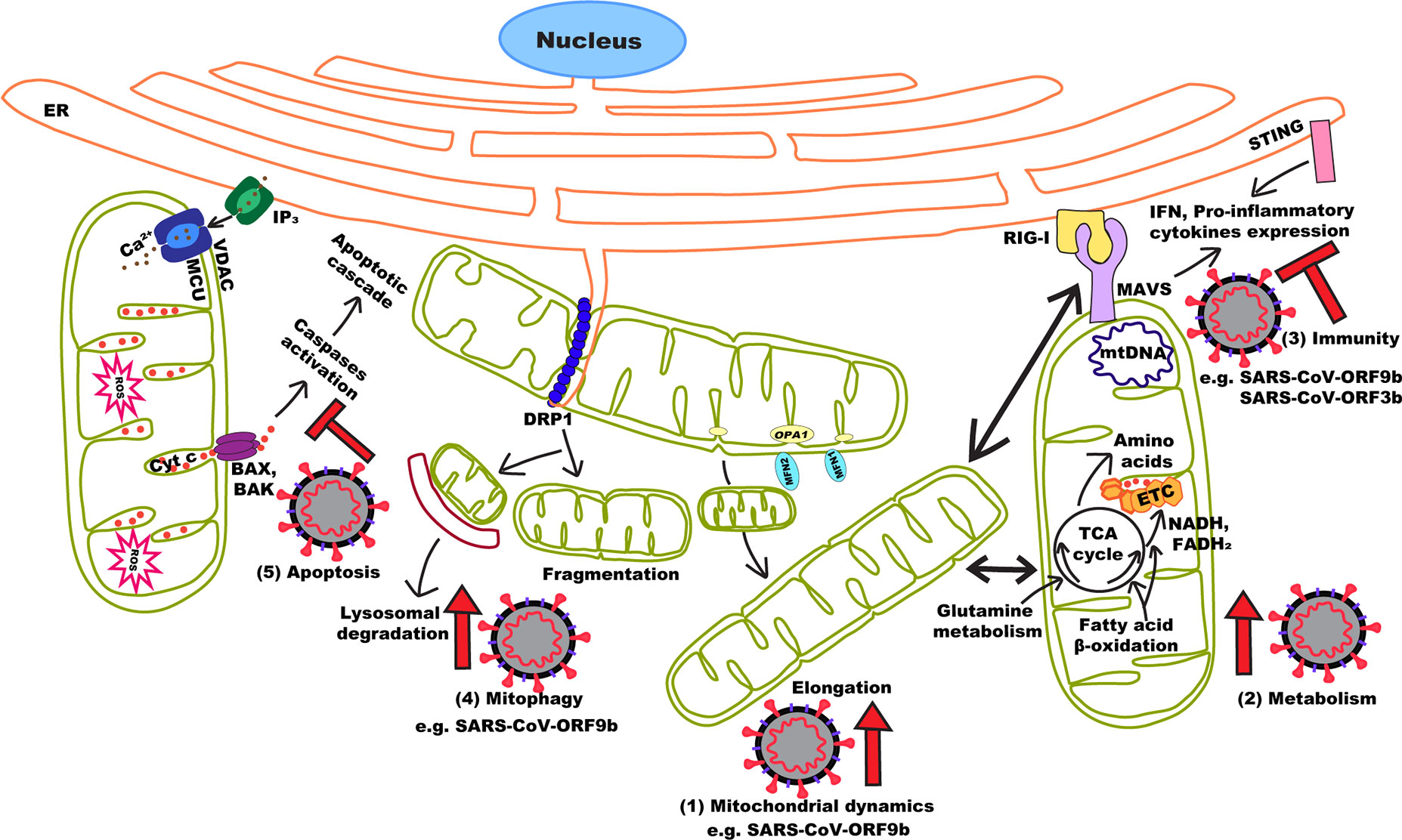
We're looking for proof of effects of the novel coronavirus(es) on mitochondria that appear to manifest the following steps shown below. Steps that relate to what the "Path Report" above was speaking to.
With all the background already offered, you'll certainly recognize the green shapes below as mitochondria. And who today wouldn't recognize that little spikey ball?
So below is a selection of some of the relevant literature: a point of contact between everything mitochondria, and everything SARS-CoV-2.
Much of this mini-bibliography has been unchanged since 2020. In some ways, that's a compliment to its robust nature!
And yet, keeping tabs on relevant publications, as time goes by, is worth doing.
So the first article is a review of the topic from 21 June, 2024.
A nice addition, particularly in the setting of "long-term" COVID-19.
Rurek M (2024), Mitochondria in COVID-19:
from cellular and molecular perspective.
Front. Physiol. 15:1406635.
doi: 10.3389/fphys.2024.1406635
The initial lines from the paper's introduction are copied below.
>"The rapid development of the COVID-19 pandemic resulted in a closer
analysis of cell functioning during β-coronavirus infection. This review will
describe evidence for COVID-19 as a syndrome with a strong, albeit still
underestimated, mitochondrial component. Due to the sensitivity of host
mitochondria to coronavirus infection, SARS-CoV-2 affects mitochondrial
signaling, modulates the immune response, modifies cellular energy
metabolism, induces apoptosis and ageing, worsening."
Mitochondria in COVID-19__from cellular and molecular perspective
> "Here, we reviewed the multitude of known strategies of coronaviruses and other viruses to usurp mitochondria-associated mechanisms involved in the host innate immune response, and put them in context with the current knowledge on SARS-CoV-2. We argue that maintenance of mitochondrial integrity is essential for adequate innate immune system responses and to blunt mitochondrial modulation by SARS-CoV-2."
Mitochondria – in the crossfire of SARS-CoV-2 and immunity
> "Viruses manipulate cellular machinery and functions to subvert intracellular environment conducive for viral proliferation. They strategically alter functions of the multitasking mitochondria to influence energy production, metabolism, survival, and immune signaling."
Mitochondrial dynamics and viral infections - A close nexus
> "Decline in mitochondrial function occurs with aging and may increase mortality.
We discuss mitochondrial contribution to Covid-19 sepsis, specifcally the complex interaction of innate immune function, viral replication, hyperinfammatory state, and HIF-α/Sirtuin pathways."
> "... we suggest how CoV-2 localization of RNA transcripts in mitochondria, hijacks the host cell’s mitochondrial function to viral advantage. Besides viral RNA transcripts, RNA also localizes to mitochondria. SARS-CoV-2 may manipulate mitochondrial function indirectly.
Decoding SARS-CoV-2 hijacking of host mitochondria in COVID-19 pathogenesis.
> "While vaccines against SARS-CoV-2 are being developed, the mechanisms through which this virus takes control of an infected cell to replicate remains poorly understood. Upon infection, viruses completely rely on host cell molecular machinery to survive and replicate. To escape from the immune response and proliferate, viruses strategically modulate cellular metabolism and alter subcellular
organelle architecture and functions. One way they do this is by modulating the structure and function of mitochondria, a critical cellular metabolic hub but also a key platform for the regulation of cellular immunity. This versatile nature of mitochondria defends host cells from viruses through several mechanisms including cellular apoptosis, ROS signaling, MAVS activation and mitochondrial DNA-dependent immune activation. These events are regulated by mitochondrial dynamics, a process by which mitochondria alter their structure (including their length and connectivity) in response to stress or other cues. It is therefore not surprising that viruses, including coronaviruses hijack these
processes for their survival."
Mitochondria Targeted Viral Replication and Survival Strategies—Prospective on SARS-CoV-2
> Next, getting more and more specific on the mitochondrial localization of the virus.
"In this study, we show that SARS-CoV 3b fused with EGFP at its N- or C- terminus co-localized with a mitochondria specific marker in some transfected cells. Mutation analysis of SARS-CoV 3b revealed that the domain spanning amino acids 80 to 138 was essential for its mitochondria localization."
Mitochondrial Location of Severe Acute Respiratory Syndrome.
> Closer and closer to understanding.
"These results indicate that SARS-CoV ORF-9b manipulates host cell mitochondria and mitochondrial function to help evade host innate immunity. This study has uncovered an important clue to the
pathogenesis of SARS-CoV infection and illustrates the havoc that a small ORF can cause in cells."
> Moving out of the lab, and closer to the patient's bedside.
"Here, we discuss various cellular and systemic incidents caused by SARS-CoV-2 that may critically
impact intra and extracellular mitochondrial function, and contribute to the progression and severity of
the disease. It is crucial to understand how these key modulators impact COVID-19 pathogenesis in
the quest to identify novel therapeutic targets that may reduce fatal outcomes of the disease."
"Despite its central role in maintaining oxidative homeostasis, and ROS generation, the mitochondrion
has received limited attention regarding its role in COVID-19 pathogenesis and management (Edeas et
al, 2020)(Keshav et al. 2020). Many questions remain unanswered about the role of the mitochondria
during the inflammatory "cytokine storm" in COVID-19 patients. Here we propose a hypothetical
scheme, based on existing evidence, describing the potential role of the inflammatory signals in
perpetuating a cycle of events that aggravate mitochondrial oxidative damage and contribute to major
systemic alterations including coagulopathy, ferreptosis and microbial dysbiosis. We propose that not
only the intracellular mitochondria dysfunction is a consequence of COVID-19 infection, but the less
explored extracellular mitochondria (specifically platelets mitochondria) may affect blood coagulation,
clot and thrombosis formation."
" Cardiolipin is a mitochondrial phospholipid which participates in the maintenance of the structural integrity of the mitochondrial membrane. The highest concentration of cardiolipin is concentrated in the monolayer of the inner mitochondrial membrane. Interestingly, serological findings of critically ill COVID-19 patients with coagulopathy and thrombocytopenia, showed the presence of anticardiolipin IgA antibodies in serum. Cardiolipin maintains the stability of cytochrome-c of the electron transport chain, however, it is also oxidation sensitive. The presence of anticardiolipin IgA antibodies may signify oxidative mitochondrial impairments associated with COVID-19 pathogenesis."
Mitochondria and Microbiota dysfunction in COVID-19 pathogenesis.
All excellent articles. Two lines were highlighted because they each relate directly to what must follow on our journey.
But here, the point of this bibliography is to find support for our hypothesis, that the patients with "long-term" COVID-19 have a mitochondrial illness, caused by SARS-CoV-2, and still symptomaticlly present after the virus is gone.
We think that there is now, through these articles (and others we will continue to place), just enough proof from the "peer-reviewed" literature for our hypothesis, to allow us to move ahead.
"Move ahead to what ?"
Well, ...
- 1.) Move ahead to preventing worse outcomes in those at greater risk for such results should they become infected. Who are they? The elderly, the overweight, those with a chronic illness like diabetes, those who work in a "high risk" setting, certain ethnic groups.
- 2.) Move ahead to curing those with the "long-term" COVID-19 clinical picture, so they can finally get over this.
- 3.) Move ahead because mitochondria are waiting. They've worked hard all their lives. They need a helping hand now. We are about to embark on compassionate care for mitochondria.
Our journey continues.
Care to come along ?
How this looks today >>>>>
<<<< Previous page
<<<< Home
A découvrir aussi
- Mitochondria : Amazing, and simply Amazing !
- Mitochondria : Get sick sometimes
- Selected Bibliography : Mitochondrial topics - background to "long-term" COVID-19